 Implanted biochips could be the tool of
Big Brother, but they are more likely to become the treatment
of choice for the physician of the 21st century.
Implanted biochips could be the tool of
Big Brother, but they are more likely to become the treatment
of choice for the physician of the 21st century.
Implanted biochips could be the tool of
Big Brother, but they are more likely to become the treatment
of choice for the physician of the 21st century.
Paranoid ranting is a staple on the internet, and the topic of biochips is a particular favorite. Biochips - any microprocessor chips that can be used in biology - mean many things to many people. The web's preachers focus on a simple idea: an implanted chip that identifies each person uniquely, and can be used to track their location.
This wonderful idea - capable of locating lost children, downed soldiers, and wandering Alzheimers patients - sounds alarming even to many mild-mannered civil libertarians. To Living Truth Ministries of Austin, TX, it is no less than "a tremendous bonanza for the coming Antichrist!" Second Advent Ministries of San Bernardino, Calif., warns us that the US social security number will soon be replaced (at the orders of the "New World Order United Nations-controlled world government", no less) by a chip-encoded "18-digit numbering system [which] will consist of THREE separate sets of SIX DIGITS each: 6-6-6! Coincidental? No. Not if you believe Bible prophecy."
Reality is somewhat less alarming. A simple ID chip is already walking around in tens of thousands of individuals, but all of them are pets. Companies such as AVID (Norco, Calif.), Electronic ID, Inc. (Cleburne, Tx.), and Electronic Identification Devices, Ltd. (Santa Barbara, Calif.) sell both the chips and the detectors. The chips are the size of an uncooked grain of rice, small enough to be injected under the skin using a syringe needle. They respond to a signal from the detector, held just a few feet away, by transmitting out an identification number. This number is then compared to database listings of registered pets.
Daniel Man, a plastic surgeon in private practice in Boca Raton, Fla., holds a patent on a more sinister device: a chip that would enable lost humans to be tracked by satellite. He has a large-scale model, but for miniaturization and regulatory approval he will need a substantial amount of cash. "There are some companies that are interested, but nothing is official," he says. "We're not giving up on it yet."
The civil liberties debate over biochips has obscured their more ethically benign and medically useful applications. Medical researchers have been working to integrate chips and people for many years, often plucking devices from well-known electronic appliances. Jeffrey Hausdorff of the Beth Israel Deaconess Medical Center (Boston, Mass.) has used the type of pressure-sensitive resistors found in the buttons of a microwave oven as stride timers. He places one sensor in the heel of a shoe, and one in the toe, and adds a computer to the ankle to calculate the duration of each stride.
"Young, healthy subjects can regulate the duration of each step very accurately," he says. But elderly patients prone to frequent falls have extremely variable stride times, a flag that could indicate the need for more strengthening exercises or a change in medication. Hausdorff is also using the system to determine the success of a treatment for congestive heart failure. By monitoring the numbers of strides that a person takes, he can directly measure the patient's activity level, bypassing the often flawed estimate made by the patient.
Hausdorff's chips are external, but a chip proposed by Sensors for Medicine and Science, Inc. (S4MS; Germantown, Md.) will be injected under the skin. The chip will allow diabetics to easily monitor the level of the sugar glucose in their blood. Diabetics currently use a skin prick and a hand-held blood test, and then medicate themselves with insulin depending on the result. The system is simple and works well, but the need to draw blood means that most diabetics don't test themselves as often as they should. Although they may get away with this in the short term, in later life those who monitored infrequently suffer from blindness, loss of circulation, and other complications.
The solution is more frequent testing, using a less invasive method. Various companies are trying to extract the required body fluid, using either an electric current (Cygnus, Inc., Redwood City, Calif.) or a tiny pore induced by a laser (SpectRx, Norcross, Ga.) or a small needle (Integ, St Paul, Minn.).
"All of these approaches ameliorate the drawing of blood," says George Daniloff, Chief Scientific Officer of S4MS, "but they still require manipulation of skin, and the skin may be perturbed." The S4MS chip, however, will sit underneath the skin, sense the glucose level, and send the result back out by radio-frequency communication.
 |
| The S4MS chip for sensing oxygen or glucose. Light generated by the light-emitting diode (LED) causes surrounding molecules to fluoresce. The light that emerges has a new wavelength, and only this light passes through the filter to be detected by the photodiode. The oxygen or glucose decreases the fluorescence of the molecules in the top reservoir. |
Glucose is detected because the sugar reduces the amount of light that the fluorescent chemical re-emits. The more glucose there is, the less light that is detected. S4MS is still developing the perfect fluorescent chemical, but the key design innovation of the S4MS chip has been fully worked out. The idea is simple: the LED is sitting in a sea of the fluorescent molecules. In most detectors the light source is far away from the fluorescent molecules, and the inefficiencies that come with that mean more power and larger devices. The prototype S4MS chip uses a 22µW LED, almost forty times less powerful than the tiny power-on buttons on a computer keyboard. The low power requirements mean that energy can be supplied from the outside, by a process called induction. The fluorescent detection itself does not consume any chemicals or proteins, so the device is self sustaining.
Daniloff has a working model of an oxygen sensor that uses the same layout. With it's current circuitry it is about the size of a large shirt-button, but the final silicon wafer will be less than a millimeter square. "The scale transition is not a challenge," says Daniloff. "The challenge is to illustrate the principle." The oxygen sensor will be useful not only to monitor breathing in intensive care units, but also to check that packages of food, or containers of semiconductors stored under nitrogen gas, remain airtight.
Tom Ferrell of the Oak Ridge National Laboratory in Oak Ridge, Tenn., is also developing an oxygen-sensing chip, but his version sends light pulses out into the body. The light is absorbed to varying extents, depending on how much oxygen is being carried in the blood, and Ferrell's chip detects the light that is left. The rushes of blood pumped by the heart are also detected, so the same chip is a pulse monitor. A number of companies already make large-scale versions of such detectors, and Ferrell says he has "collaborated with almost every company in this area," although he will not name names.
Ferrell estimates that the oxygen chip is two years away, but he has already reduced the dimensions of his temperature-sensing chip to 3mm per side. The transition of certain semiconductors to their conducting state is inherently sensitive to temperature, so designing the sensor was simple enough. With some miniature radio-frequency transmitters, and foam-rubber earplugs to hold the chip in place, the device is complete. Ferrell sees applications for anyone from sick children, to chemotherapy patients who can be plagued by sudden rises in body temperature in response to their anti-cancer drugs.
Sensing and measuring is one thing, but can we switch the body on and off? Heart pacemakers use the crude approach: large jolts of electricity to synchronize the pumping of the heart. The electric pulses of the Activa implant, made by Medtronic, Inc. (Minneapolis, Minn.), are directed not at the heart but the brain. They turn off brain signals that cause the uncontrolled movements, or tremors, associated with diseases such as Parkinson's.
Drug therapy for Parkinson's disease aims to replace the brain messenger dopamine, a product of the brain cells that are dying. But eventually the drug's effects wear off, and the erratic movements come charging back. "I've had patients tell me that they scare their grandkids because they are flaying around like a fish," says Gary Heit, a neurosurgeon at Stanford University Medical Center. "Imagine your whole body twisted like a charleyhorse."
 |
| The Activa implant for Parkinson's disease tremors. Driven by a pulse generator implanted in the chest, the implant delivers high frequency stimulation to an area of the brain called the thalamus. Image courtesy of Medtronic, Inc. |
The Activa implant interferes with aberrant brain functioning. The most ambitious bioengineers are trying to add back brain functions, restoring sight and sound where there was darkness and silence.
 |
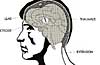
| The Clarion cochlear implant. Sound is received by a microphone, processed by a minicomputer (not shown), and the electric signals are transmitted to the implant by radio-frequency communication. After decoding of the signal, the multiple electrodes directly activate nerve cells that communicate information about sound to the brain. Image courtesy of Advanced Bionics Corp. |
The cochlear implant delivers electrical pulses directly to the nerve cells in the cochlea, the spiral-shaped structure that translates sound into nerve pulses. In normal hearing individuals, sound waves set up vibrations in the walls of the cochlea, and hair cells detect these vibrations. High frequency noises (deep notes) vibrate the base of the cochlea, while low frequency notes vibrate nearer the top of the spiral. The implant mimics the job of the hair cells. It splits the frequencies of incoming noises into a number of channels (typically eight), and then stimulates the appropriate part of the cochlea.
 |
| The circuitry of the implanted part of the cochlear implant, including the radio-frequency receivers. Image courtesy of Advanced Bionics Corp. |
The result is a broad-brush version of hearing. While some recipients of the devices report speech-like sounds, many characterize their new world as being populated with legions of quacking ducks or banging garbage cans. But the success is undeniable. "Currently two thirds to three quarters of patients [with more recent models] can understand speech without lip-reading," says Steve Rebscher, a member of the UCSF team. "It's pretty amazing, and certainly better than a lot of people anticipated these devices would do."
With the ear at least partially conquered, the next logical target is the eye. Several groups are working on implantable chips that mimic the action of photoreceptors, the light-sensing cells at the back of the eye. Photoreceptors are lost in both retinitis pigmentosa, a genetic disease, and age-related macular degeneration, the most common cause of lost sight in the developed world.
|
| The logic circuit for the retinal implant made by Joseph Rizzo and John Wyatt. Ten thousand transistors are packed on this circuit, which is just 2mm on each side. |
For now the power supply comes from a wire inserted directly into the eye and, using this device, Rizzo has detected signals reaching the brain. "We know we can get visual information to the brain," he says, "but we don't know what kind of vision that will result in."
Eugene de Juan of Johns Hopkins Wilmer Eye Institute (Baltimore, Md.) is trying to answer that question by using human subjects. His electrodes, inserted directly into the eye, are large and somewhat crude. But his results have been startling. Completely blind patients have seen well-defined flashes, which change in position and brightness as de Juan changes the position of the electrode or the amount of current. In his most recent experiments, patients have identified simple shapes outlined by multiple electrodes. With as little as an 8 x8 array, de Juan believes he could approximate character recognition, and a 25 x 25 array might give a crude image.
The big money in eye implants is in Germany, where the government has pledged ~$10 million to two projects. One is similar to the US projects, in which chips are implanted on the surface of the retina, the structure at the back of the eye. The other project is putting its implants at the back of the retina, where the photoreceptors are normally found. These 'subretinal' chips may block the transport of oxygen and food to the overlying nerve cells, so Eberhart Zrenner of the University of Tübingen, Germany, is developing 'chain mail' electrode arrays, with plenty of holes for the delivery of supplies.
The subretinal approach more closely mimics the action of the lost photoreceptors. The chip delivers its message at the source, before intervening layers of retinal nerve cells do some complicated processing. Rizzo thinks that his chip's hardware will be able to compensate for these computations, but for now he has other things to worry about. "There are all sorts of processes that go on that we're just going to ignore initially," he says. As with the cochlear implant, he says, "the biological tests will show you the best way to stimulate. Ultimately the only thing that matters is what the person sees."
The first big test - showing that a remotely powered device can give true visual signals - is yet to be done. "We haven't got to first base yet," says Rizzo, "but we're close." With a working device many years away, Rizzo is a model of caution. "It's always better to talk down the possibilities than to talk them up, because there are many reasons why the implants might fail," he says. "This is science fiction stuff."